




Abstract
Objective:
While the deleterious associations of surgical menopause following bilateral oophorectomy withcardiovascular disease are documented, less is specifically known concerning subclinical atherosclerosis progression.
Methods:
We used data from 590 healthy postmenopausal women randomized to hormone therapy or placebo in the Early vs. Late Intervention Trial with Estradiol (ELITE), which was conducted from July 2005 to February 2013. Subclinical atherosclerosis progression was measured as annual rate of change in carotid artery intima-media thickness (CIMT) over a median 4.8 years. Mixed-effects linear models assessed the association of hysterectomy and bilateral oophorectomy compared to natural menopause with CIMT progression adjusted for age and treatment assignment. We also tested modifying associations by age at or years since oophorectomy or hysterectomy.
Results:
Among 590 postmenopausal women, 79 (13.4%) underwent hysterectomy with bilateral oophorectomy and 35 (5.9%) underwent hysterectomy with ovarian conservation; a median of 14.3 years prior to trial randomization. Compared with natural menopause, women who underwent hysterectomy with and without bilateral oophorectomy had higher fasting plasma triglycerides while women who underwent bilateral oophorectomy had lower plasma testosterone. The CIMT progression rate in bilaterally oophorectomized women was 2.2 μm/year greater than natural menopause (p=0.08); specifically, compared to natural menopause, the associations were significantly greater in postmenopausal women who were more than 50 years old at the time of bilateral oophorectomy (p=0.014) and in postmenopausal women who underwent bilateral oophorectomy more than 15 years prior to randomization (p=0.015). Moreover, the CIMT progression rate in hysterectomized women with ovarian conservation was 4.6 μm/year greater than natural menopause (p=0.015); in particular, compared to natural menopause, the association was significantly greater in postmenopausal women who underwent hysterectomy with ovarian conservation more than 15 years prior to randomization (p=0.018).
Conclusions:
Hysterectomy with bilateral oophorectomy and ovarian conservation were associated with greater subclinical atherosclerosis progression relative to natural menopause. The associations were stronger for later age and longer time since oophorectomy/hysterectomy. Further research should continue to examine long-term atherosclerosis outcomes related to oophorectomy/hysterectomy.
Keywords: bilateral oophorectomy, hysterectomy, subclinical atherosclerosis, cardiovascular disease, clinical trial, sex hormones
Introduction
About 400,000 bilateral oophorectomies with concurrent hysterectomies are performed annually in the United States1. While this surgical procedure can prevent ovarian cancer, bilateral oophorectomy comes with risks regardless of timing relative to age. Women who undergo bilateral oophorectomy before menopause experience an abrupt decline in various sex steroid hormones and disruption of the hypothalamic-pituitary-ovarian axis2. Postmenopausal women also suffer from testosterone deficiency after oophorectomy3.
A large body of literature shows that oophorectomized women experience an increased risk of several adverse outcomes in the short- and long-term4–8. In particular, after decades of follow-up, two population-based cohort studies showed that oophorectomized women had a higher incidence of and mortality due to cardiovascular diseases (CVD) compared with naturally postmenopausal women4,8. A cross-sectional study reported that carotid artery intima-media thickness (CIMT) was significantly positively associated with years since oophorectomy9. Although these studies highlighted the deleterious associations of bilateral oophorectomy with cardiovascular conditions, few studies have attempted to quantify the longitudinal association of subclinical atherosclerosis progression with bilateral oophorectomy. In particular, possible modification of longitudinal associations by age at bilateral oophorectomy or years since bilateral oophorectomy, have not been reported. Furthermore, the current literature lacks sufficient data on the association between hysterectomy with ovarian conservation and subclinical atherosclerosis progression in postmenopausal women, highlighting a significant gap in knowledge. Our study aims to address this gap by providing novel insights into these associations and adding to the existing literature on the cardiovascular risks associated with surgical menopause.
We studied 590 healthy postmenopausal women from the Early vs. Late Intervention Trial with Estradiol (ELITE). The objective of this post-trial analysis was to investigate the association of subclinical atherosclerosis progression with type of menopause (hysterectomy with or without bilateral oophorectomy vs. natural menopause). Additionally, the association between subclinical atherosclerosis progression and hysterectomy with or without bilateral oophorectomy in postmenopausal women was evaluated in relation to timing of oophorectomy: 1) Age at which women underwent bilateral oophorectomy or hysterectomy without oophorectomy; and 2) Number of years since women underwent bilateral oophorectomy or hysterectomy without oophorectomy.
Methods
Study design and population
Baseline and on-trial measurements of clinical features and serum hormone levels were obtained from 590 healthy menopausal women who participated in ELITE, a randomized, double-blinded, placebo-controlled clinical trial conducted from July 2005 to February 201310. Eligible participants included postmenopausal women who had not had regular menses for more than 6 months and were either <6 years or ≥10 years since menopause at the time of randomization, free of clinical evidence of CVD and with a serum estradiol level less than 25 pg/ml11. Women were excluded from the trial if they had unknown time since menopause, had fasting plasma triglyceride levels >500 mg/dL, diabetes mellitus or fasting serum glucose levels >140 mg/dL, serum creatinine level >2.0 mg/L, had uncontrolled hypertension, thyroid disease, or life-threatening disease with prognosis less than 5 years, or had a history of deep vein thrombosis, pulmonary embolism, or breast cancer.
At study enrollment, time since menopause was obtained and categorized as early postmenopause (<6 years) or late postmenopause (≥10 years). This stratification was based on the hypothesis tested in ELITE that initiation of HT within 6 years following menopause is associated with reduced atherosclerosis progression while initiation of HT more than 10 years since menopause has null or unfavorable effects atherosclerosis progression10. After stratifying by early and late postmenopause, participants were randomly assigned to receive oral 17β-estradiol (1 mg per day) or placebo in a 1:1 allocation ratio. Women who had an intact uterus additionally received 4% micronized progesterone (45 mg) vaginal gel or placebo for 10 days for each 30-day cycle; women who did not have an intact uterus in the placebo group received a placebo gel. The treatment assignments were blinded from participants, investigators, imaging specialists and data monitors.
Following randomization, participants returned to the study clinic every month for the first six months and then every other month until completion of the trial10,12. The median number of years of post-randomization follow-up was 4.8 (range, 0.5 to 6.7 years). Plasma and serum samples were collected and stored at −80°C at baseline and follow-up visits every six months. Fasting levels of total plasma triglycerides, total cholesterol, and high-density lipoprotein cholesterol levels were measured by enzymatic assays and standardized to the CDC according to the Lipid Research Clinic protocol. Low-density lipoprotein-cholesterol was computed using the Friedewald equation13. Concentrations of sex steroid hormones and sex steroid binding globulin (SHBG) were measured from serum samples at baseline, 12 and 36 months during the trial. Serum levels of testosterone, estrone and estradiol were quantified by validated radioimmunoassays (RIAs)14. Free and bioavailable estradiol and testosterone were calculated from derived equations15,16 using a validated algorithm17.
Reproductive history
At baseline, participants provided detailed information of their reproductive history using a structured questionnaire including age at menarche, date of last menstrual period, number of pregnancies and deliveries, age at first and last pregnancies and deliveries, prior contraceptive, and HT use (ever use, duration and dose), date of hysterectomy, whether women underwent oophorectomy at the time of hysterectomy and number of ovaries removed. Medical records were reviewed to confirm the self-reported information concerning removal of ovary/ovaries. No women underwent oophorectomy during participation in ELITE.
Assessment of CIMT
High-resolution B-mode ultrasound imaging and standardized procedures for longitudinally imaging and measuring arterial wall thickness were utilized to assess CIMT of the right distal common carotid artery. The B-mode ultrasound images for CIMT measurements were obtained at two baseline examinations prior to randomization and at subsequent clinical visits every 6 months during the trial follow-up for longitudinal measures of subclinical atherosclerosis10.
Other covariate information
Participating women were randomly assigned to treatment (active, placebo) according to time since menopause strata (<6 years or ≥10 years). Weight and height were measured at baseline and all subsequent clinical visits to calculate BMI (kg/m2).
Statistical analysis
Continuous variables were reported as median (IQR) and compared among menopause groups using the Kruskal-Wallis test. Categorical variables were summarized as frequency (percent) and chi-square tests used for group comparisons. Correlations between continuous variables were assessed by Pearson’s correlation.
To measure rate of CIMT progression over study follow-up, mixed-effects linear models with per-participant repeated measures of CIMT as the dependent variable and time (years) since randomization as the independent variable were constructed. The regression coefficient for time estimated the average per-participant annual rate of change in CIMT. A participant-specific intercept (baseline CIMT) and slope (rate of change in CIMT) were included as random effects in the mixed model. CIMT progression was compared among women who had prior concurrent hysterectomy and bilateral oophorectomy with women who underwent natural menopause. In the primary analyses, a two-way interaction term between years since randomization and hysterectomy/oophorectomy status was used to assess whether menopausal women with a prior concurrent hysterectomy and bilateral oophorectomy, or with a prior hysterectomy with ovarian conservation or unilateral oophorectomy, had different CIMT progression rates compared to naturally postmenopausal women. In the secondary analyses, we included interaction terms of years since randomization with age at bilateral oophorectomy/hysterectomy or years since bilateral oophorectomy/hysterectomy. These interaction terms tested for differences in CIMT progression rate by age at bilateral oophorectomy/hysterectomy (≤50 years old; >50 years old) and by time since bilateral oophorectomy/hysterectomy (≤15 years; >15 years), compared to naturally menopausal women. We used the Wald test to further test whether the effect estimates (the rate of change in CIMT) differed by age at bilateral oophorectomy/hysterectomy (>50 years old versus ≤50 years old) and time since bilateral oophorectomy/hysterectomy (>15 years versus ≤15 years). All models were adjusted for age, BMI, time since menopause (< 6 years, ≥ 10 years), and treatment assignment (active, placebo) in the multivariable analyses. In further analysis, we included a three-way interaction term between on-trial treatment assignment, years since randomization, and hysterectomy/oophorectomy status or age at bilateral oophorectomy or years since oophorectomy to test whether the association between oophorectomy and CIMT progression was modified by on-trial hormone therapy.
In ELITE, a total of 643 eligible women were randomly assigned to either HT or to placebo. The analysis was restricted to 590 women (5,550 clinical visits) after exclusion of 47 women without CIMT measurements during the trial, 1 woman who reported a hysterectomy but did not know whether her ovaries were removed, and 5 women who reported unilateral oophorectomy without concurrent hysterectomy.
All statistical analyses were performed using Stata Version 16.1 (College, Station, TX), reporting 2-sided p-values, with a significance level of p < 0.05.
Results
Among 590 women included in the analyses, 79 (13.4%) underwent concurrent hysterectomy and bilateral oophorectomy before the trial started. The median (IQR) age at bilateral oophorectomy was 45.9 (8.3) years; years since bilateral oophorectomy was 14.3 (12.2) years. CIMT was measured 9.4 times on average across the various groups and was equitable among the three groups (data not shown). Women who had hysterectomy with ovarian conservation or unilateral oophorectomy were older (median=67.3 years) than women who had concurrent hysterectomy and bilateral oophorectomy (median=60.8 years) or women who had natural menopause (median=59.3 years, Table 1). These three groups were relatively homogenous with respect to race, education, history of smoking, and alcohol intake.
Table 1.
Baseline Characteristics and Reproductive History in ELITE Women (N=590)
| Variables | Naturally Menopausal (n=476) | Hysterectomizeda (n=35) | Bilaterally Oophorectomizedb (n=79) | Total | P-value |
|---|---|---|---|---|---|
| Demographic characteristics | |||||
| Age (years) | 59.3 (8.9) | 67.3 (8.9) | 60.8 (8.4) | 60.0 (9.3) | <0.001 |
| Treatment Assignment | |||||
| Hormone Therapy | 273 (49.8) | 22 (62.9) | 36 (45.6) | 295 (50.0) | 0.23 |
| Placebo | 239 (50.2) | 13 (37.1) | 43 (54.4) | 295 (50.0) | |
| Race | 0.55 | ||||
| White Non-Hispanic | 331 (69.4) | 22 (66.8) | 57 (72.2) | 410 (69.5) | |
| Black Non-Hispanic | 39 (8.2) | 5 (14.3) | 7 (8.8) | 61 (8.6) | |
| Hispanic | 62 (13.0) | 7 (20.0) | 10 (12.7) | 79 (13.4) | |
| Asian or Pacific Islander | 44 (9.24) | 1 (2.9) | 5 (6.3) | 50 (8.5) | |
| Education | 0.63 | ||||
| High school graduate or less | 17 (3.6) | 2 (5.7) | 3 (3.8) | 22 (3.7) | |
| Trader/business school/some college | 132 (27.7) | 11 (31.4) | 28 (35.4) | 171 (29.0) | |
| Bachelor’s degree/graduate/professional education | 327 (68.7) | 22 (62.9) | 48 (60.8) | 397 (67.3) | |
| Smoking | 0.87 | ||||
| Never | 285 (59.9) | 21 (60.0) | 47 (59.5) | 353 (59.8) | |
| Former | 174 (36.5) | 13 (37.1) | 31 (39.2) | 218 (37.0) | |
| Current | 17 (3.6) | 1 (2.9) | 1 (1.3) | 10 (3.2) | |
| Alcohol intake per day | 0.74 | ||||
| None | 245 (51.5) | 17 (48.6) | 36 (45.6) | 298 (50.5) | |
| 1 | 169 (35.5) | 13 (37.1) | 29 (36.7) | 211 (35.8) | |
| 2 | 47 (9.9) | 5 (14.3) | 10 (12.7) | 62 (10.5) | |
| ≥2 | 15 (3.1) | 0 (0.0) | 4 (5.0) | 19 (3.2) | |
| Reproductive History | |||||
| Age at bilateral oophorectomy | ‐‐ | ‐‐ | 45.9 (8.3) | ‐‐ | ‐‐ |
| Years since oophorectomy | ‐‐ | ‐‐ | 14.3 (12.2) | ‐‐ | ‐‐ |
| Age started menstrual (years) | 13.0 (2.0) | 13.0 (1.0) | 12.0 (2.0) | 13.0 (2.0) | 0.034 |
| Number of pregnancies | 2.0 (3.0) | 3.0 (2.0) | 2.0 (3.0) | 2.0 (3.0) | 0.47 |
| Number of deliveries | 2.0 (2.0) | 2.0 (2.0) | 2.0 (2.0) | 2.0 (2.0) | 0.15 |
| Age at first pregnancy (years) | 24.0 (8.0) | 24.0 (9.0) | 21.0 (6.0) | 24.0 (8.0) | <0.001 |
| Age at last pregnancy (years) | 32.0 (10.0) | 29.0 (6.0) | 28.0 (7.0) | 31.0 (10.0) | <0.001 |
| Previous hormone use | <0.001 | ||||
| No | 158 (33.2) | 1 (2.9) | 5 (6.3) | 164 (27.8) | |
| Yes | 318 (66.8) | 34 (97.1) | 74 (93.7) | 426 (72.2) | |
| Duration of hormone use (years) | 5.0 (7.0) | 14.0 (12.0) | 11.0 (9.0) | 7.0 (9.0) | <0.001 |
| Previous oral contraceptives use | 0.26 | ||||
| No | 386 (81.4) | 25 (71.4) | 60 (76.9) | 471 (80.2) | |
| Yes | 88 (18.6) | 10 (28.6) | 18 (23.1) | 116 (19.8) | |
| Duration of oral contraceptives use (years) | 7.0 (8.0) | 5.5 (7.0) | 9.5 (10.5) | 7.0 (8.0) | 0.17 |
Numbers in the table are median (IQR) for continuous variables, count (%) for categorical variables.
P-values by Kruskal-Wallis test for continuous variables; by chi-square test for binary/categorical variables
ELITE = Early vs. Late Intervention Trial with Estradiol; -- not applicable
Includes women who reported having hysterectomy with ovarian conservation (n=26) or unilateral oophorectomy (n=9)
Includes women who reported having concurrent hysterectomy and bilateral oophorectomy
Women who underwent hysterectomy with or without bilateral oophorectomy were more likely to be in the late postmenopause stratum (≥10 years), to have used HT, and to have had a longer duration of past HT use (Table 2). Compared to naturally postmenopausal women, hysterectomized women with or without a concurrent bilateral oophorectomy had higher triglycerides at baseline (p=0.003 among the 3 groups). The mean serum testosterone level at baseline was lowest in women who underwent concurrent hysterectomy and oophorectomy (p=0.009 among the 3 groups). Estradiol, estrone and SHBG levels were not different among the 3 groups. Age at bilateral oophorectomy and years since bilateral oophorectomy were highly inversely correlated (r = - 0.63).
Table 2.
Baseline Clinical Features and Steroid Hormone Levels in ELITE Women (N=590)
| Variables | Naturally Menopausal (n=476) | Hysterectomizeda (n=35) | Bilaterally Oophorectomizedb (n=79) | Total | P-value |
|---|---|---|---|---|---|
| Clinical Features | |||||
| Menopause stratum | <0.001 | ||||
| <6years | 233 (49.0) | 3 (8.6) | 9 (11.4) | 245 (41.5) | |
| ≥10years | 243 (51.0) | 32 (91.4) | 70 (88.6) | 345 (58.5) | |
| Carotid intima-media thickness (μm) | 746 (126.3) | 781.5 (111.3) | 744 (104.5) | 746.5 (123.8) | 0.57 |
| Systolic blood pressure (mmHg) | 116.8 (15.8) | 117.7 (14.7) | 118.7 (16.3) | 117.3 (16.3) | 0.18 |
| BMI (kg/m2) | 26.1 (7.0) | 27.9 (7.1) | 27.3 (8.0) | 26.4 (7.3) | 0.26 |
| HDL cholesterol (mg/dl) | 63.5 (23.0) | 59.0 (22.0) | 62.5 (28.0) | 63.5 (23.5) | 0.36 |
| LDL cholesterol (mg/dl) | 133.7 (41.5) | 135.3 (43.2) | 130.6 (41.9) | 133.6 (41.6) | 0.55 |
| Triglycerides (mg/dl) | 90 (55.0) | 119 (68.0) | 98.5 (60.5) | 91.5 (58.5) | 0.003 |
| Glucose (mg/dl) | 81.3 (11.3) | 85.1 (14.1) | 81.9 (12.1) | 81.6 (11.6) | 0.39 |
| Antihypertensive medication | |||||
| Yes | 104 (21.8) | 8 (22.9) | 26 (32.9) | 138 (23.4) | 0.10 |
| Antihyperlipidemic medication | |||||
| Yes | 93 (19.5) | 9 (25.7) | 18 (22.8) | 120 (20.0) | 0.58 |
| Steroid Hormone Levels | |||||
| Estradiol (pg/mL) | 11.0 (6.9) | 11.1 (8.7) | 11.2 (6.5) | 11.0 (7.0) | 0.94 |
| Free estradiol (pg/mL) | 0.3 (0.2) | 0.3 (0.2) | 0.3 (0.2) | 0.3 (0.2) | 0.83 |
| Bioavailable estradiol (pg/mL) | 6.6 (4.7) | 6.9 (5.3) | 6.9 (5.1) | 6.6 (4.8) | 0.83 |
| Estrone (pg/mL) | 17.4 (10.4 | 19.1 (15.2) | 18.3 (8.6) | 17.6 (10.4) | 0.56 |
| Testosterone (ng/dL) | 31.0 (16.8) | 30.5 (23.7) | 27.0 (14.9) | 30.3 (17.1) | 0.009 |
| Free testosterone (ng/dL) | 5.5 (3.5) | 4.7 (3.6) | 4.7 (2.8) | 5.3 (3.4) | 0.12 |
| Bioavailable testosterone (ng/dL) | 13.4 (8.6) | 11.5 (8.9) | 11.5 (6.8) | 13.0 (8.4) | 0.12 |
| SHBG (nmol/liter) | 56.3 (35.1) | 50.6 (37.7) | 51.9 (30.6) | 55.6 (34.1) | 0.32 |
Numbers in the table are median (IQR) for continuous variables, count (%) for categorical variables.
P-values by Kruskal-Wallis test for continuous variables; by chi-square test for binary/categorical variables
BMI = body mass index; ELITE = Early versus Late Intervention Trial with Estradiol; HDL= high density lipoprotein; LDL = low density lipoprotein; SHBG = sex hormone binding globulin.
Includes women who reported having hysterectomy with ovarian conservation (n=26) or unilateral oophorectomy (n=9)
Includes women who reported having concurrent hysterectomy and bilateral oophorectomy
Mean baseline CIMT in oophorectomized women did not differ from naturally menopausal women (p=0.82). Mean baseline CIMT was approximately 31 μm lower in hysterectomized women with one or both intact ovaries than naturally menopausal women adjusted for age, although the difference was not statistically significant (p=0.09, Table 3). Further adjustment for duration of past hormone use did not substantially alter the baseline CIMT or conclusions for either oophorectomy or hysterectomy alone group (data not shown). Over a median of 4.68 years of follow-up, women with concurrent hysterectomy and bilateral oophorectomy had a greater annual CIMT progression rate than naturally menopausal women, and the difference was marginally statistically significant [β coefficient = 2.49 (95% CI: −0.054 to 5.04) μm CIMT per year; p=0.055]. Compared with naturally menopausal women, women who underwent hysterectomy with ovarian conservation or unilateral oophorectomy prior to randomization also had a significantly greater annual CIMT progression rate [β coefficient = 4.57 (95% CI: 0.87–8.26) μm CIMT per year; p=0.015, Table 3 & Figure 1]. The positive difference in mean CIMT progression rate between women who underwent hysterectomy with ovarian conservation and naturally menopausal women indicated a worse progression in mean CIMT. In further analyses of CIMT progression by age at and time since oophorectomy, mean CIMT progression rate was significantly greater in women more than 50 years old at time of bilateral oophorectomy, compared with women who experienced natural menopause (p=0.033, Table 4a). The difference in mean CIMT progression rate between women who underwent bilateral oophorectomy above age 50 and naturally menopausal women was 5.29 μm per year (95% CI: 0.42–10.15). The mean CIMT progression rate was 1.58 μm per year greater (95% CI: −1.31 to 4.48) in women at age 50 years or younger at time of bilateral oophorectomy than naturally menopausal women; the difference in CIMT progression was not statistically significant (p=0.28). The mean CIMT progression rate did not between women who underwent bilateral oophorectomy above age 50 and at age 50 years or younger (p=0.56).
Table 3.
Evaluation of Oophorectomy Status Associated with CIMT Progression Rate (μm/y) From Mixed Effects Linear Regression Analysisa (N=590)
| Variables | Regression Coefficient [95% CI] | P-valueb |
|---|---|---|
| Baseline mean CIMT (μm) compared to naturally postmenopausal women: | ||
| Hysterectomized women with or without unilateral oophorectomy | −30.40 | 0.09 |
| [−65.87 to 5.07] | ||
| Hysterectomized women with bilateral oophorectomy | 2.89 | 0.82 |
| [−21.77 to 27.54] | ||
| Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.19 | <0.001 |
| [6.22 to 8.16] | ||
| Difference in CIMT rate compared to naturally postmenopausal women (μm/year): | ||
| Hysterectomized women with or without unilateral oophorectomy | 4.57 | 0.015 |
| [0.87 to 8.26] | ||
| Hysterectomized women with bilateral oophorectomy | 2.49 | 0.055 |
| [−0.05 to 5.04] |
CIMT = carotid artery intima-media thickness
The reference group are women who had natural menopause.
Models adjusted for age (years), treatment assignment (hormone therapy, placebo), BMI, and time since menopause (< 6 years, ≥ 10 years).
P-values from the Wald test.
Figure 1. Differential Timing of Bilateral Oophorectomy Association with CIMT Progression Rate (μm/y).

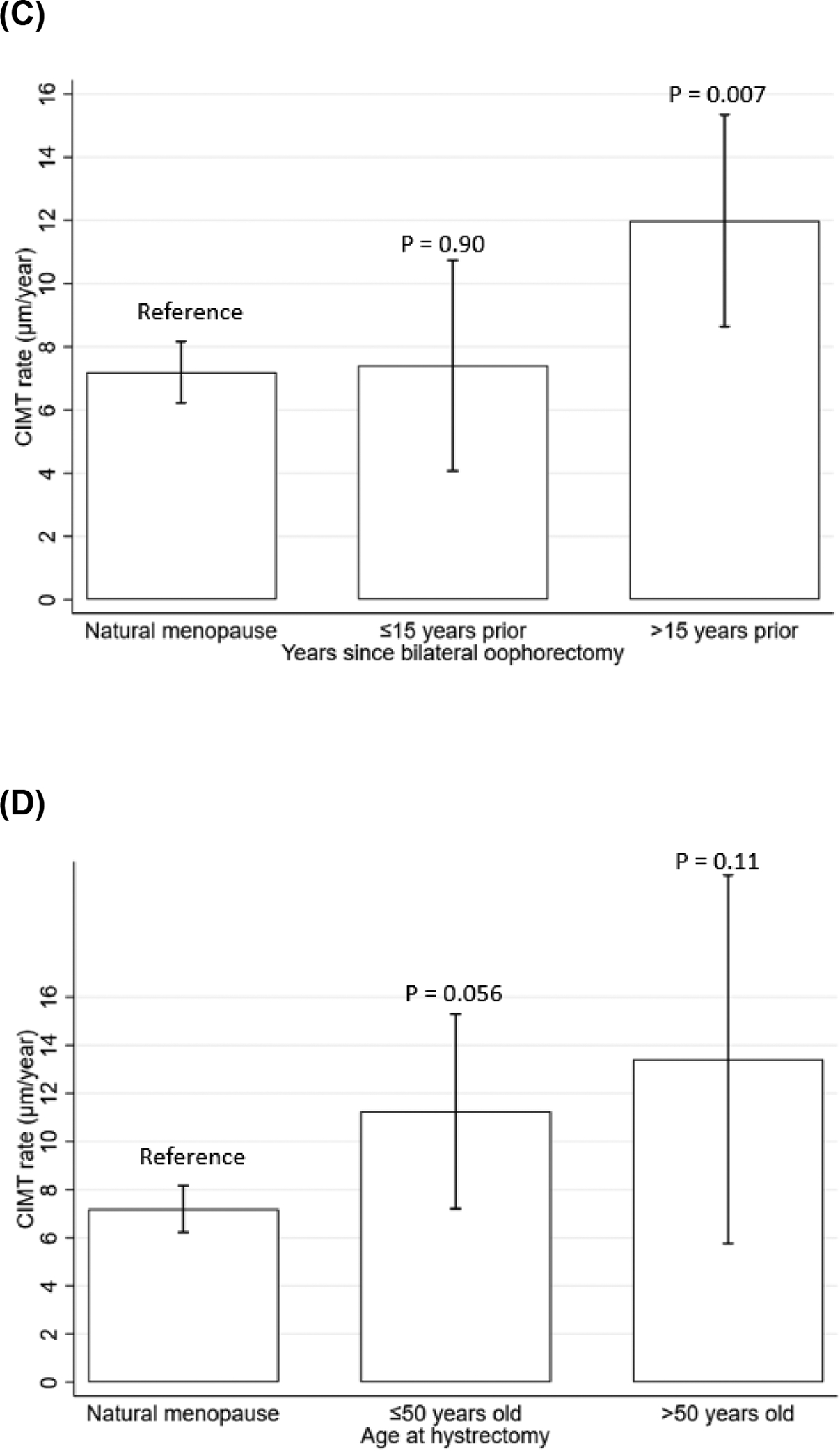

A. compared women who underwent concurrent bilateral oophorectomy and hysterectomy, and women who underwent hysterectomy with ovarian conservation, with naturally postmenopausal women.
B. compared women who had bilateral oophorectomy ≤50 years old, and >50 years old with naturally menopausal women.
C. compared women who had bilateral oophorectomy ≤15 years and >15 years prior to randomization with naturally menopausal women.
D. compared women who had hysterectomy with ovarian conservation ≤50 years old, and >50 years old with naturally menopausal women.
E. compared women who had hysterectomy with ovarian conservation ≤15 years and >15 years prior to randomization with naturally menopausal women.
The mean CIMT progression rate in each stratum was calculated from mixed-effects models with adjustment for age (years), treatment assignment (hormone therapy, placebo), BMI, and time since menopause (< 6 years, ≥ 10 years).
Lines indicate 95% confidence intervals of the mean CIMT progression rate (μm/y); P-value from the Wald test.
Table 4a.
Evaluation of Oophorectomy Status (Bilateral Oophorectomy (n=79) vs Natural Menopause (n=476)) Association with CIMT Progression Rate (μm/y) From Mixed Effects Linear Regression Analysisa (N=555)
| Model 1 Bilateral oophorectomy vs natural menopause | Model 2 Age at bilateral oophorectomy vs natural menopause | Model 3 Years since bilateral oophorectomy vs natural menopause | ||||||
|---|---|---|---|---|---|---|---|---|
| Regression coefficient [95% CI] | P-valueb | Regression coefficient [95% CI] | P-valueb | Regression coefficient [95% CI] | P-valueb | |||
| Baseline mean CIMT (μm) compared to naturally postmenopausal women: | Baseline mean CIMT (μm) compared to naturally postmenopausal women: | Baseline mean CIMT (μm) compared to naturally postmenopausal women: | ||||||
| Oophorectomy strata | 3.10 | 0.81 | Oophorectomy ≤50 years old | −3.83 | 0.79 | Oophorectomy ≤15 years | 11.71 | 0.48 |
| [−21.72 to 27.91] | [−31.82 to 24.16] | [−21.02 to 44.44] | ||||||
| Oophorectomy >50 years old | 24.02 | 0.31 | Oophorectomy >15 years | −6.37 | 0.72 | |||
| [−22.24 to 70.29] | [−40.54 to 27.80] | |||||||
| Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.19 | <0.001 | Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.19 | <0.001 | Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.19 | <0.001 |
| [6.22 to 8.17] | [6.22 to 8.16] | [6.22 to 8.16] | ||||||
| Difference in CIMT rate compared to naturally postmenopausal women (μm/year) in: | Difference in CIMT rate compared to naturally postmenopausal women (μm/year) in: | Difference in CIMT rate compared to naturally postmenopausal women (μm/year) in: | ||||||
| Oophorectomy strata | 2.49 | 0.056 | Oophorectomy ≤50 years old | 1.58 | 0.28 | Oophorectomy ≤15 years | 0.22 | 0.90 |
| [−0.07, to .05] | [−1.31 to 4.48] | [−3.26 to 3.69] | ||||||
| Oophorectomy >50 years old | 5.29c | 0.033 | Oophorectomy >15 years | 4.79d | 0.007 | |||
| [0.42 to 10.15] | [1.31 to 8.28] | |||||||
CIMT = carotid artery intima-media thickness
The reference group are women who had natural menopause.
Model 1: compared bilaterally oophorectomized women with naturally postmenopausal women.
Model 2: compared women who had bilateral oophorectomy ≤50 years old, and >50 years old with naturally menopausal women.
Model 3: compared women who had bilateral oophorectomy ≤15 years and >15 years prior to randomization with naturally menopausal women.
Models adjusted for age (years), treatment assignment (hormone therapy, placebo), BMI, and time since menopause (< 6 years, ≥ 10 years).
P-values from the Wald test.
The difference in mean CIMT progression rate was not statistically different between women who underwent bilateral oophorectomy above age 50 and at age 50 years or younger (p=0.56).
The difference in mean CIMT progression rate was not statistically different between women who underwent bilateral oophorectomy more than 15 years and at or within 15 years prior to randomization (p=0.71).
These findings by age at hysterectomy were similar in women who underwent hysterectomy with ovarian conservation (Table 4b, Model 4). Compared to naturally menopausal women, mean CIMT progression was non-significantly greater in both women who were above age 50 [β coefficient = 4.06 (95% CI: −0.10 to 8.22) μm CIMT per year, p = 0.056] and at or below age 50 [β coefficient = 6.21 (95% CI: −1.50 to 13.92) μm CIMT per year, p = 0.11] at time of hysterectomy.
Table 4b.
Evaluation of Hysterectomy Status (Hysterectomy with Ovarian Conservation (n=35) vs Natural Menopause (n=476)) Association with CIMT Progression Rate (μm/y) From Mixed Effects Linear Regression Analysisa (N=511)
| Model 4 Age at hysterectomy vs natural menopause | Model 5 Years since hysterectomy vs natural menopause | ||||
|---|---|---|---|---|---|
| Regression coefficient [95% CI] | P-valueb | Regression coefficient [95% CI] | P-valueb | ||
| Baseline mean CIMT (μm) compared to naturally postmenopausal women: | Baseline mean CIMT (μm) compared to naturally postmenopausal women: | ||||
| Hysterectomy ≤50 years old | −31.68 | 0.11 | Hysterectomy ≤15 years | −28.31 | 0.45 |
| [−70.16 to 6.80] | [−101.57 to 44.97] | ||||
| Hysterectomy >50 years old | −42.63 | 0.26 | Hysterectomy >15 years | −35.31 | 0.08 |
| [−116.42 to 31.16] | [−74.20 to 3.59] | ||||
| Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.20 | <0.001 | Annual rate of CIMT progression in naturally postmenopausal women (μm/year) | 7.20 | <0.001 |
| [6.22 to 8.17] | [6.22 to 8.17] | ||||
| Difference in CIMT rate compared to naturally postmenopausal women (μm/year) in: | Difference in CIMT rate compared to naturally postmenopausal women (μm/year) in: | ||||
| Hysterectomy ≤50 years old | 4.06 | 0.056 | Hysterectomy ≤15 years | 2.72 | 0.49 |
| [−0.10 to 8.22] | [−4.99 to10.42] | ||||
| Hysterectomy >50 years old | 6.21 | 0.11 | Hysterectomy >15 years | 5.04 | 0.018 |
| [−1.50 to 13.92] | [0.88 to 9.19] | ||||
CIMT = carotid artery intima-media thickness
The reference group are women who had natural menopause.
Model 4: compared women who had hysterectomy with ovarian conservation ≤50 years old, and >50 years old with naturally menopausal women.
Model 5: compared women who had hysterectomy with ovarian conservation ≤15 years and >15 years prior to randomization with naturally menopausal women.
Models adjusted for age (years), treatment assignment (hormone therapy, placebo), BMI, and time since menopause (< 6 years, ≥ 10 years).
P-values from the Wald test.
The difference in mean CIMT progression rate was not statistically different between women who underwent hysterectomy with ovarian conservation above age 50 and at age 50 years or younger (p=0.16).
The difference in mean CIMT progression rate was not statistically different between women who underwent hysterectomy with ovarian conservation more than 15 years and at or within 15 years prior to randomization (p=0.16).
Women who underwent bilateral oophorectomy more than 15 years prior to randomization had a significantly greater mean CIMT progression rate than women who experienced natural menopause (p=0.007, Table 4a). The difference in mean CIMT progression rate between women who underwent bilateral oophorectomy more than 15 years prior to randomization and women who experienced natural menopause was 4.79 μm per year (95% CI: 1.31–8.28, p = 0.007). The CIMT progression rate did not differ between women who underwent bilateral oophorectomy at or within 15 years prior to randomization and women who experienced natural menopause [β coefficient = 0.22 (95% CI: −3.26 to 3.69) μm CIMT per year; p=0.90]. The mean CIMT progression rate was not statistically different between women who underwent bilateral oophorectomy more than 15 years and at or within 15 years prior to randomization (p=0.71).
The findings by years since hysterectomy were similar in women who underwent hysterectomy with ovarian conservation (Table 4b, Model 5). Compared to naturally menopausal women, mean CIMT progression was statistically significantly greater in women who underwent hysterectomy more than 15 years prior to randomization [β coefficient = 5.04 (95% CI: 0.88–9.19) μm CIMT per year; p=0.018]. The mean CIMT progression at or within 15 years at time of hysterectomy [β coefficient = 2.72 (95% CI: −4.99 to 10.42) μm CIMT per year] was also greater than naturally menopausal women but the difference was not statistically significant (p=0.49).
The effect estimates in the multivariable models remained the same after further adjustment for duration of past hormone therapy (data not shown). Associations of CIMT progression rate with hysterectomy/oophorectomy status, age at bilateral oophorectomy or years since oophorectomy were not significantly different between the HT and the placebo groups (data not shown).
Discussion
A few cross-sectional studies investigated whether CIMT measurements differed between surgically and naturally postmenopausal women but yielded conflicting results from no association to positive association of CIMT levels with surgical menopause18–20. Comparable with those findings, baseline CIMT levels were not associated with oophorectomy status in the ELITE sample. In longitudinal analyses, ELITE women who underwent bilateral oophorectomy prior to study involvement tended to have elevated atherosclerosis progression compared with women who experienced natural menopause (β coefficient = 2.49 (95% CI: −0.054 to 5.04) μm CIMT per year; p=0.055). Specifically, our findings suggest that older age at oophorectomy and extended years following oophorectomy may have more detrimental associations than oophorectomy itself with rates of atherosclerosis progression. We observed that women who underwent bilateral oophorectomy above 50 years of age or more than 15 years prior randomization had significantly greater CIMT progression than women who experienced natural menopause. Further adjustment for duration of past hormone therapy did not alter the effect estimates or conclusions. Furthermore, we found that the two subgroups were relatively distinct; only two women had both a later age at oophorectomy and longer duration since oophorectomy. These results suggest that later age at oophorectomy and longer duration since oophorectomy may be independent risk factors for subclinical atherosclerosis.
In this ELITE sample, testosterone levels were 14.8% lower in women who underwent oophorectomy than in women with intact ovaries (with or without hysterectomy). Both short- and long-term testosterone reduction following oophorectomy has been reported in other studies21,22. In women undergoing oophorectomy, a considerable pre- to two-week post-surgery reduction in testosterone levels was found in both premenopausal (40.3% reduction) and postmenopausal (32.7% reduction) women21. The authors concluded that ovaries not only serve as an essential source of testosterone production in the premenopausal phase but remain important in secreting steroid hormones in postmenopausal women. In a pooled analysis of over 6000 postmenopausal women from 13 studies, testosterone concentrations were 30% lower in oophorectomized women over a decade after bilateral oophorectomy compared with women with intact ovaries22. Similar reductions were also found in circulating androstenedione and DHEAS, whereas the concentrations of estradiol and estrone were not significantly different between oophorectomized and naturally postmenopausal women22.
Limited studies have investigated the associations between testosterone and CVD in women, with conflicting findings regarding whether testosterone is harmful or beneficial. It has been speculated that excess testosterone levels in women may negatively affect the cardiovascular system23. In this regard, several studies reported that endogenous total or bioavailable testosterone levels were positively associated with CVD risk factors, including obesity, insulin resistance, and diabetes in postmenopausal women. However, it is unknown whether testosterone was a marker or mediator of CVD in those studies and there are no solid data suggesting that excess total testosterone increases cardiovascular risk and mortality among postmenopausal women24,25. On the other hand, recent studies showed that low testosterone levels in women may contribute to greater atherosclerosis risk23,26,27. One mechanism suggests higher testosterone levels have a beneficial effect on endothelial function in postmenopausal women due to androgen receptor expression in the vasculature24. In this respect, it is worth noting that circulating sex steroid hormone levels may not reflect blood vessel aromatase concentration or function. Another potential mechanism involves aromatase conversion of testosterone to estradiol in the vasculature in which beneficial effects of testosterone are expressed through estradiol on cardiovascular function28. A recent cohort study of 639 postmenopausal women (mean age, 73.8) with a 20-year follow-up may explain the conflicting results as to whether testosterone is harmful or beneficial, showing that an optimal range of testosterone may exist since both high and low extremes of testosterone levels were related to elevated CVD risk24. Women in the lowest quintile of total testosterone (≤80 pg/ml) were at 62% (95% CI, 1.10–2.39) higher risk of incident coronary heart disease (CHD) while women in the highest 20% of bioavailable testosterone (≥63 pg/ml) were at 96% higher risk of CHD, compared with women who were in middle quintiles of total or bioavailable testosterone levels. The persistent testosterone reduction resulting from bilateral oophorectomy may contribute to an elevated risk of CVD. Several studies have reported that bilateral oophorectomy is linked to other unfavorable CVD risk profiles, including increased BMI and systolic blood pressure and elevated total and LDL-cholesterol, which contribute to elevated CVD risk29–31.
Compared with our study, the Estrogen in the Prevention of Atherosclerosis Trial (EPAT) shared uniform data collection and measures; EPAT targeted postmenopausal women with baseline low-density lipoprotein cholesterol levels of 130 mg/dL or greater32. In EPAT, mean age-adjusted CIMT levels at baseline were significantly higher in oophorectomized women relative to naturally postmenopausal women, but this difference was statistically non-significant after adjusting for years since menopause33. In the current study, mean CIMT levels at baseline did not differ between oophorectomized women and women who experienced natural menopause. In EPAT, the associations between oophorectomy and CIMT progression were not assessed; as such, we were not able to compare the results.
In the current study, the elevated CIMT progression rate relative to natural menopause was most apparent in women who had undergone bilateral oophorectomy, more than 15 years prior to randomization. A recent longitudinal study that used data from the Women’s Isoflavone Soy Health (WISH) trial showed that CIMT progression in oophorectomized women was greater than in women who experienced natural menopause. Consistent with ELITE findings, WISH showed that among women who experienced menopause more than 10 years prior to randomization, the rate of CIMT progression significantly doubled in oophorectomized women relative to women with intact ovaries; there was no significant finding in women who experienced menopause 5–10 years prior to randomization34 Our finding is also consistent with an early autopsy study showing that bilaterally oophorectomized women were more likely to show severe coronary atherosclerosis a decade following surgery compared to women with natural menopause35. However, the difference in atherosclerosis blockage was not apparent in women who had bilateral oophorectomy within ten years of autopsy. This research was restricted to white women over 40 years old, including those who underwent oophorectomy after 50 years of age but never received hormone therapy as well as their naturally menopausal comparators who were matched on age and a 5-year interval of death. Although autopsy studies provide valuable measurements of coronary artery atherosclerosis when imaging tools were not yet available, autopsy studies are likely subject to bias. For example, necropsies were conducted by different individuals over the two decades of the study and lacked central validation, which could introduce nondifferential information bias in the classification of coronary artery disease. Moreover, selection of ovary-retaining controls in this study was restricted to individuals who died from cancer or automobile accidents, which may not be representative of coronary artery disease in the general population.
Prior studies investigating the associations of oophorectomy with incident diseases and mortality were more often focused on women who underwent oophorectomy before age 50 and experienced early or premature menopause5,8,36. The focus on younger women was due to the previous notion that ovaries completely lost function after menopause and no longer provided any protective effects on cardiovascular health34. However, emerging data show that intact ovaries become a crucial source for maintaining androgen levels in the bloodstream in older women as the adrenal glands less efficiently secrete androgens with aging22,34,37. A few studies assessed effects of oophorectomy in older women to provide more information to assist decision-making regarding prophylactic removal of ovaries3. These studies reported an increased risk of first myocardial infarction in women who underwent oophorectomy between age 50 and 55, compared with women with ovarian conservation3,38. This is consistent with our finding of increased atherosclerosis progression in women who underwent oophorectomy relative to natural menopause that was more apparent in women who underwent oophorectomy above 50 years of age.
Consistent with findings of bilateral oophorectomy, the elevated CIMT progression rate relative to natural menopause was also observed in our small sample of 35 women who had undergone hysterectomy with ovarian conservation, particularly those who had more than 15 years prior to randomization. The Women’s Health Initiative (WHI) Observational Study reported that women who underwent hysterectomy only had higher total mortality and fatal and nonfatal CVD compared to naturally postmenopausal women39,40. However, a subsequent report using the WHI observational data suggested that adding bilateral salpingo-oophorectomy (BSO) during hysterectomy may not result in further risks compared to hysterectomy alone40. Preserving the ovaries during a hysterectomy may nonetheless lead to compromised ovarian function, possibly due to the disturbance of ovarian blood supply during the surgical procedure40. Our study was not sufficiently powered to differentiate the individual contributions of bilateral oophorectomy and hysterectomy to the observed increase in subclinical atherosclerosis progression, thus making it challenging to determine whether the greater atherosclerosis progression observed in women undergoing these surgical interventions is mainly attributed to oophorectomy, hysterectomy, or both. Further research is needed to disentangle the potential independent effects of these two surgical procedures on cardiovascular health outcomes.
One of the limitations of our study is that there is no information as to why participants chose to undergo hysterectomy and bilateral oophorectomy. According to a historical cohort study, women who underwent oophorectomy for benign ovarian conditions before age 50 had a significantly higher risk of coronary artery disease, congestive heart failure, and chronic obstructive pulmonary disease compared with women without benign ovarian conditions over approximately 14 years of follow-up4. It remains unknown whether bilateral oophorectomy itself or the indications for surgery that lead to oophorectomy place women at a greater risk of subclinical atherosclerosis and cardiovascular diseases. Although we queried women regarding their past use of steroid hormones prior to the trial, we did not systematically collect information on the timing, duration or specific form of past hormone use or whether women started hormone therapy immediately after undergoing bilateral oophorectomy. Another limitation is that the relatively small number of oophorectomized women reduced statistical power. Moreover, majority of participants in the trial were healthy and well-educated women, which could potentially limit the generalizability of the findings to the broader population of postmenopausal women. Despite these limitations, this study is one of the few longitudinal studies to assess associations of hysterectomy with or without oophorectomy with progression of atherosclerosis. The associations of age at oophorectomy and years since oophorectomy with atherosclerosis progression investigated in this study provide additional information for decision-making concerning prophylactic oophorectomy. Additional human studies assessing subclinical atherosclerosis progression with extended follow-up after bilateral oophorectomy are required to confirm our findings.
Conclusion
Our study suggests that women who undergo hysterectomy with ovarian conservation or bilateral oophorectomy may experience greater subclinical atherosclerosis progression compared to those who experience natural menopause, with a stronger association observed in older women and those with a longer time since surgery. Although our study did not differentiate the independent contributions of oophorectomy and hysterectomy to subclinical atherosclerosis progression, it provides valuable insights into the potential cardiovascular risks associated with surgical menopause. Our findings contribute to the growing body of literature on the cardiovascular consequences of oophorectomy/hysterectomy. Our findings further highlight the need for careful consideration of the benefits and risks of these procedures in clinical practice and may inform clinical decision-making for women with gynecological conditions. Future research in this area will advance our understanding of the long-term cardiovascular risks associated with these surgical interventions.
Sources of funding:
This work was supported by the National Institute on Aging, National Institutes of Health (R01-AG024154 and R01-AG059690).
Footnotes
This work was presented as an oral presentation at the North American Menopause Society annual meeting, Oct 13–15, 2022, Atlanta, Georgia.
Clinical trial registration: ClinicalTrials.gov, NCT00114517.
Financial disclosures/Conflicts of interest: None reported.
References
- 1.Moore BJ, Steiner CA, Davis PH, Stocks C, Barrett ML. Trends in hysterectomies and oophorectomies in hospital inpatient and ambulatory settings, 2005–2013. Published online 2016. http://hcupnet.ahrq.gov/. [PubMed]
- 2.Rocca WA, Grossardt BR, Shuster LT. Oophorectomy, menopause, estrogen, and cognitive aging: The timing hypothesis. In: Neurodegenerative Diseases. Vol 7.; 2010:163–166. doi: 10.1159/000289229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Parker WH, Broder MS, Liu Z, Shoupe D, Farquhar C, Berek JS. Ovarian conservation at the time of hysterectomy for benign disease. Clin Obstet Gynecol. 2007;50(2):354–361. [DOI] [PubMed] [Google Scholar]
- 4.Rocca WA, Gazzuola-Rocca L, Smith CY, et al. Accelerated accumulation of multimorbidity after bilateral oophorectomy: a population-based cohort study. Mayo Clin Proc. 2016;91(11):1577–1589. doi: 10.1016/j.mayocp.2016.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rivera CM, Grossardt BR, Rhodes DJ, et al. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause. 2009;16(1):15–23. doi: 10.1097/gme.0b013e31818888f7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rocca WA, Grossardt BR, Geda YE, et al. Long-term risk of depressive and anxiety symptoms after early bilateral oophorectomy. Menopause. 2018;25(11):1275–1285. doi: 10.1097/GME.0000000000001229 [DOI] [PubMed] [Google Scholar]
- 7.Kurita K, Henderson VW, Gatz M, et al. Association of bilateral oophorectomy with cognitive function in healthy, postmenopausal women. Fertil Steril. 2016;106(3):749–756.e2. doi: 10.1016/j.fertnstert.2016.04.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Parker WH, Feskanich D, Broder MS, et al. Long-term mortality associated with oophorectomy compared with ovarian conservation in the Nurses’ Health Study. Obstetrics and Gynecology. 2013;121(4):709–716. doi: 10.1097/AOG.0b013e3182864350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dwyer KM, Nordstrom CK, Merz CNB, Dwyer JH. Carotid wall thickness and years since bilateral oophorectomy the Los Angeles Atherosclerosis Study. Am J Epidemiol. 2002;156(5):438–444. doi: 10.1093/aje/kwf051 [DOI] [PubMed] [Google Scholar]
- 10.Hodis HN, Mack WJ, Henderson VW, et al. Vascular effects of early versus late postmenopausal treatment with estradiol. New England Journal of Medicine. 2016;374(13):1221–1231. doi: 10.1056/nejmoa1505241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hodis HN, Mack WJ, Shoupe D, et al. Methods and baseline cardiovascular data from the Early versus Late Intervention Trial with Estradiol testing the menopausal hormone timing hypothesis. Menopause. 2015;22(4):391–401. doi: 10.1097/GME.0000000000000343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sriprasert I, Hodis HN, Karim R, et al. Differential effect of plasma estradiol on subclinical atherosclerosis progression in early vs late postmenopause. Journal of Clinical Endocrinology and Metabolism. 2018;104(2):293–300. doi: 10.1210/jc.2018-01600 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Freidewald WT LRFD. Estimation of the concentration of Low density lipoprotein cholesterol in plasma without the use of the preparative ultracentrifuge. Clin Chem. Published online 1972:499–502. [PubMed] [Google Scholar]
- 14.Goebelsmann U, Horton R, Mestman JH, et al. Male pseudohermaphroditism due to testicular 17β-hydroxysteroid dehydrogenase deficiency1. J Clin Endocrinol Metab. 1973;36(5):867–879. doi: 10.1210/jcem-36-5-867 [DOI] [PubMed] [Google Scholar]
- 15.Södergard R, Bäckström T, Shanbhag V, Carstensen H. Calculation of free and bound fractions of testosterone and estradiol-17β to human plasma proteins at body temperature. J Steroid Biochem. 1982;16(6):801–810. doi: 10.1016/0022-4731(82)90038-3 [DOI] [PubMed] [Google Scholar]
- 16.Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999;84(10):3666–3672. doi: 10.1210/jcem.84.10.6079 [DOI] [PubMed] [Google Scholar]
- 17.Rinaldi S, Geay A, Déchaud H, et al. Validity of free testosterone and free estradiol determinations in serum samples from postmenopausal women by theoretical calculations. Cancer Epidemiol Biomarkers Prev. 2002;11(10 Pt 1):1065–1071. [PubMed] [Google Scholar]
- 18.Stöckl D, Peters A, Thorand B, et al. Reproductive factors, intima media thickness and carotid plaques in a cross-sectional study of postmenopausal women enrolled in the population-based KORA F4 study. BMC Womens Health. 2014;14(1). doi: 10.1186/1472-6874-14-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Özkaya E, Çakr E, Okuyan E, Çakr C, Üstün G, Küçüközkan T. Comparison of the effects of surgical and natural menopause on carotid intima media thickness, osteoporosis, and homocysteine levels. Menopause. 2011;18(1):73–76. doi: 10.1097/gme.0b013e3181e5046d [DOI] [PubMed] [Google Scholar]
- 20.Mack WJ, Slater CC, Xiang M, Shoupe D, Lobo RA, Hodis HN. Elevated subclinical atherosclerosis associated with oophorectomy is related to time since menopause rather than type of menopause. doi: 10.1016/j.fertnstert.2004 [DOI] [PubMed] [Google Scholar]
- 21.Stanczyk FZ, Chaikittisilpa S, Sriprasert I, Rafatnia A, Nadadur M, Mishell DR. Circulating androgen levels before and after oophorectomy in premenopausal and postmenopausal women. Climacteric. 2019;22(2):169–174. doi: 10.1080/13697137.2018.1535584 [DOI] [PubMed] [Google Scholar]
- 22.Key TJ, Appleby PN, Reeves GK, et al. Circulating sex hormones and breast cancer risk factors in postmenopausal women: Reanalysis of 13 studies. Br J Cancer. 2011;105(5):709–722. doi: 10.1038/bjc.2011.254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sievers C, Klotsche J, Pieper L, et al. Low testosterone levels predict all-cause mortality and cardiovascular events in women: A prospective cohort study in German primary care patients. Eur J Endocrinol. 2010;163(4):699–708. doi: 10.1530/EJE-10-0307 [DOI] [PubMed] [Google Scholar]
- 24.Laughlin GA, Goodell V, Barrett-Connor E. Extremes of endogenous testosterone are associated with increased risk of incident coronary events in older women. Journal of Clinical Endocrinology and Metabolism. 2010;95(2):740–747. doi: 10.1210/jc.2009-1693 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mcgrath KC, Mcrobb LS, Heather AK, Heather A. Androgen therapy and atherosclerotic cardiovascular disease. Vasc Health Risk Manag. 2008;4(1):11–21. [PMC free article] [PubMed] [Google Scholar]
- 26.Montalcini T, Gorgone G, Gazzaruso C, Sesti G, Perticone F, Pujia A. Role of endogenous androgens on carotid atherosclerosis in non-obese postmenopausal women. Nutrition, Metabolism and Cardiovascular Diseases. 2007;17(10):705–711. doi: 10.1016/j.numecd.2006.09.007 [DOI] [PubMed] [Google Scholar]
- 27.Montalcini T, Gorgone G, Gazzaruso C, Sesti G, Perticone F, Pujia A. Endogenous testosterone and endothelial function in postmenopausal women. Pathophysiology and natural history. 2007;18(1):9–13. [DOI] [PubMed] [Google Scholar]
- 28.Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ. 2017;8(1):33. doi: 10.1186/s13293-017-0152-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.de Kat AC, Dam V, Onland-Moret NC, Eijkemans MJC, Broekmans FJM, van der Schouw YT. Unraveling the associations of age and menopause with cardiovascular risk factors in a large population-based study. BMC Med. 2017;15(1). doi: 10.1186/s12916-016-0762-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gibson CJ, Thurston RC, el Khoudary SR, Sutton-Tyrrell K, Matthews KA. Body mass index following natural menopause and hysterectomy with and without bilateral oophorectomy. Int J Obes. 2013;37(6):809–813. doi: 10.1038/ijo.2012.164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.van Bommel MHD, de Jong MA, Steenbeek MP, et al. No signs of subclinical atherosclerosis after risk-reducing salpingo-oophorectomy in BRCA1/2 mutation carriers. J Cardiol. 2021;77(6):570–575. doi: 10.1016/j.jjcc.2020.11.005 [DOI] [PubMed] [Google Scholar]
- 32.Hodis HN, Mack WJ, Lobo RA, et al. Estrogen in the prevention of atherosclerosis. Ann Intern Med. 2001;135(11):939–953. [DOI] [PubMed] [Google Scholar]
- 33.Mack WJ, Slater CC, Xiang M, Shoupe D, Lobo RA, Hodis HN. Elevated subclinical atherosclerosis associated with oophorectomy is related to time since menopause rather than type of menopause. Fertil Steril. 2004;82(2). doi: 10.1016/j.fertnstert.2004 [DOI] [PubMed] [Google Scholar]
- 34.Mucowski SJ, Mack WJ, Shoupe D, Kono N, Paulson R, Hodis HN. Effect of prior oophorectomy on changes in bone mineral density and carotid artery intima-media thickness in postmenopausal women. Fertil Steril. 2014;101(4):1117–1122. doi: 10.1016/j.fertnstert.2013.12.055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Parrish HM, Carole Carr DA, David Hall MG, King TM. Time interval from castration in premenopausal women to development of excessive coronary atherosclerosis. Am J Obstet Gynecol. 1967;99(2). doi: 10.1016/0002-9378(67)90314-6 [DOI] [PubMed] [Google Scholar]
- 36.Rocca WA, Rocca LG, Smith CY, et al. Loss of ovarian hormones and accelerated somatic and mental aging. Physiology. 2018;33(6):374–383. doi: 10.1152/physiol.00024.2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kotsopoulos J, Shafrir AL, Rice M, et al. The relationship between bilateral oophorectomy and plasma hormone levels in postmenopausal women. Horm Cancer. 2015;6(1):54–63. doi: 10.1007/s12672-014-0209-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Shoupe D, Parker WH, Broder MS, Liu Z, Farquhar C, Berek JS. Elective oophorectomy for benign gynecological disorders. Menopause. 2007;14(3):580–585. doi: 10.1097/gme.0b013e31803c56a4 [DOI] [PubMed] [Google Scholar]
- 39.Howard B v., Kuller L, Langer R, et al. Risk of cardiovascular disease by hysterectomy status, with and without oophorectomy: The Women’s Health Initiative Observational Study. Circulation. 2005;111(12):1462–1470. doi: 10.1161/01.CIR.0000159344.21672.FD [DOI] [PubMed] [Google Scholar]
- 40.Jacoby VL, Grady D, Wactawski-Wende J, et al. Oophorectomy vs Ovarian Conservation With Hysterectomy: Cardiovascular Disease, Hip Fracture, and Cancer in the Women’s Health Initiative Observational Study. Arch Intern Med. 2011;171(8):760–768. https://jamanetwork.com/ [DOI] [PubMed] [Google Scholar]